Doctor Chettawut’s Non-Penile Inversion SRS Technique
Dr. Chettawut’s non-penile inversion technique is a one-stage male-to-female sex reassignment surgery (SRS) that provides the best possible vulva appearance, sexual pleasure, and physiological function of the vagina.
Detailed Process of Creating Each Part of the Female Genital Organ
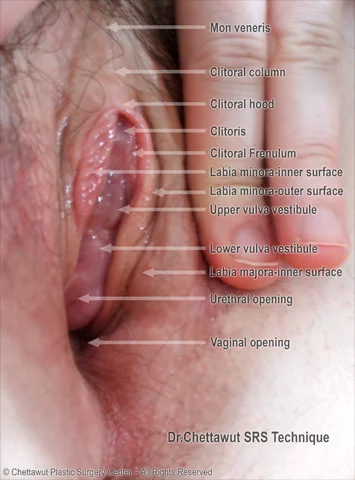
1. Mons Veneris
The mons veneris, also known as the mons pubis in females, is a rounded mound over the pubic bone. Its size varies with the amount of fat tissue, sensitive to estrogen. Post-SRS, the mons veneris contains the neurovascular pedicle, responsible for making the clitoris and parts of the vulva vestibule sensitive.
2. Clitoral Hood
The clitoral hood is a fold of skin that surrounds and protects the clitoris, playing a vital role in achieving pleasure during sexual arousal. Dr. Chettawut preserves the special sensory nerve innervating this structure, using the pink-colored foreskin (prepuce) for a natural appearance.
3. Clitoris
Made from the most sensitive part of the glans penis, the clitoris is set in the correct anatomical position. It is designed to resemble a female clitoris, with the option for a slightly larger size if requested. Dr. Chettawut guarantees the ability to achieve orgasm due to the preservation of the dorsal nerve of the clitoris.